What is an Hysterectomy?
A hysterectomy is a surgical procedure to remove the uterus.
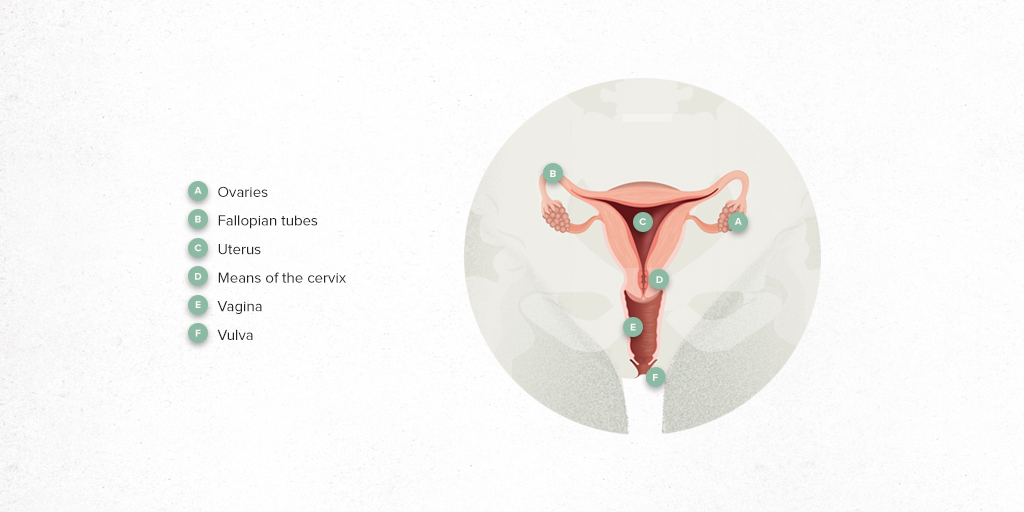
In most cases, the uterus (body and cervix) is completely removed; this is called a total hysterectomy. A subtotal hysterectomy is when the main body of the womb is removed, leaving the cervix in place.
Currently, both fallopian tubes are usually removed (salpingectomy) in conjunction with the hysterectomy procedure.
Performing a hysterectomy does not involve removal of the ovaries. The ovaries may be removed, depending on aspects such as the age of the patient and the presence of associated ovarian pathology.
How it is performed?
A hysterectomy is the most common gynaecological surgical procedure in the world. It can be done via any of the usual access routes in gynaecology, which are:
Vaginal hysterectomy: the uterus is removed through the vagina, which leaves no abdominal scars. This is the route of choice and the most common for uterine prolapse surgery (the pelvic floor muscles weaken and no longer adequately support the uterus).
Abdominal hysterectomy: access is through the abdomen. There are different modalities of abdominal surgery practised today, which are:
-
Open surgery: this involves a wide, vertical incision in the abdomen, above the pubis and below the navel. This is usually done for women with a large volume uterus or cancer, in some cases.
-
Laparoscopic surgery: a minimally invasive technique in which small incisions are made in the abdominal wall that allow access to a thin tube called a laparoscope. The tube has a camera attached that sends images to a screen. This allows the surgeon to see inside the pelvis. For this surgery, a pneumoperitoneum is performed; that is, the abdominal cavity is filled with gas (CO₂). This is the technique used most today, due to the advantages it offers patients: less pain, better recovery, reduced hospitalisation and less risk of complications.
-
Robotic surgery: here, small incisions are also made in the abdominal wall, through which robotic arms are placed that direct the surgical instruments (e.g. scalpel and forceps) inside the pelvis. These arms are remotely controlled by the surgeon.
When is a hysterectomy done?
A hysterectomy is done in cases of benign or malignant gynaecological pathology; that is, where there are malignant tumours (cancer) or other types of diseases.
It is considered the definitive treatment for benign diseases which do not respond to drug treatment or are not well tolerated, especially when the patient has uterine bleeding and pelvic pain. It is also given to patients with no desire for children or uterine preservation.
The main diseases requiring a hysterectomy are:
-
Uterine fibroids (benign tumours): this is the most common indication for a hysterectomy.
-
Endometriosis.
-
Uterine Prolapse.
-
Abnormal Uterine Bleeding.
-
Pelvic pain.
-
Gynaecological cancer: Ovary, endometrium or cervix.
How should you prepare?
This is major surgery; so indications will be given by the nursing, anaesthesia and surgery teams. The preparation procedure for the most common operation consists of:

Preoperative tests. These include a blood test and an autologous blood donation, in case a transfusion is needed.

Electrocardiogram and/or chest x-ray, according to the age of the patient.

Low-residue diet. This is low in fibre, fat and lactose and must be followed for 5 days before entering the operating room.

Fasting on the day of surgery.
How long does it last?
Most laparoscopic abdominal hysterectomies take 60-90 minutes. Vaginal hysterectomies tend to be shorter, around 60 minutes.
However, in calculating the total surgery time, it must be borne in mind that it depends on different factors: the reason for the hysterectomy, if it is associated with other procedures, the uterine volume or other reasons that could increase the surgery time.
What happens during the operation?
Upon arrival in the operating room, the prophylactic antibiotic is given about 30 minutes before the start of the surgery through the line previously placed in the hospital ward.
General anaesthesia is required for an abdominal hysterectomy (open, laparoscopic or robotic); while locoregional anaesthesia (perispinal) can be given for the vaginal route.
Once the anaesthesia is administered, the area where the operation will be performed is disinfected with antiseptic solution. A bladder catheter is inserted that will be removed postoperatively.
Surgery consists of the coagulation and sectioning of the veins, arteries and ligaments that anchor the uterus to the pelvis, so the uterus can be extracted later. It is customary to remove it from the vagina opening; however, depending on the patient characteristics (e.g. vaginal deliveries or age) or if the uterus is very large, extraction can be performed minimally by enlarging the umbilical orifice.
The team performing the operation is usually made up of 3 gynaecologists, an anaesthetist, an anaesthesia nurse, a scrub nurse and a circulating nurse.
What happens after the hysterectomy?
After the surgery, the patients are left in the hospital ward.
After 6-8 hours, they can eat by mouth again, the urinary catheter is removed and gradually they can begin to move.
In general, hospital discharge is 24-48 hours if the surgery has been done vaginally and laparoscopically, and 3-4 days if it has been done through the open abdominal route.
If the patient has an oncological disease or if a highly complex hysterectomy has been carried out, the hospital stay may be longer.
It is customary to advise rest for about 4 weeks. During this time, you should not lift anything heavy, have sexual intercourse or take vaginal douches until the gynaecological control visit, when the healing process will be evaluated.
Remember, most patients do not have their ovaries removed; therefore, the patient will stop menstruating permanently but will continue to have normal hormonal cycles until physiological menopause.
What are the benefits of Hysterectomy?
Immediately, the hysterectomy means the cessation of menstruation, so we eliminate problems of uterine bleeding, anemia and pelvic pain, as well as problems related to oncological pathology. In this way, many women experience a significant improvement in their quality of future life.
Will I be able to take my medication?
All the patient's usual medication should be maintained until the time of surgery, providing there is no specific indication otherwise from the anaesthesia or gynaecology team.
If the patient has been prescribed a specific gynaecological treatment (generally hormonal) to treat the symptoms that motivate the hysterectomy, this should also be maintained until the day of surgery. After surgery, most hormonal treatments can be suppressed or modified.
What are the potential complications?
Hysterectomy is one of the most commonly performed pelvic surgeries in the world. Today, thanks to minimally invasive techniques such as laparoscopy and robotics, it is considered a safe surgery due to its high success rate and low incidence of complications. Mortality associated with hysterectomy remains less than 1% in most cases.
The most common complications include:

Bleeding which may, in many cases, require an iron supplement to be taken for mild postoperative anaemia. In more severe cases, a transfusion or even a reoperation may be required.

Wound infection.

Dome haematoma (which can be superinfected). Bleeding associated with the healing process of the vagina.

Urine infections.

Injury to neighbouring organs. This would be one of the most serious complications: ureteral, bladder, rectal injuries. Later, fistula complications in the form of vesico-vaginal, recto-vaginal fistula much less frequent.
What are the recommendations for a correct physical and emotional recovery after surgery?
Physically, recovery involves rest, pain control through analgesia, and early mobilization to prevent complications such as deep vein thrombosis (DVT).
In some cases, it is also recommended that, once the postoperative healing process has been completed, pelvic floor physiotherapy to strengthen the pelvic muscles and prevent urinary or sexual dysfunction.
On an emotional level, the patient is encouraged to express her concerns and must receive the necessary guidance to understand the long-term benefits of the surgery.
Does hysterectomy affect sexual function?
Many women fear that hysterectomy will affect their sexual function due to a misunderstanding of female pelvic anatomy, associating it with the loss of a woman's entire hormonal system. Hysterectomy results in the cessation of menstruation mediated by the uterus, but in most women with benign indications, it is not associated with the removal of the ovaries (which are responsible for hormonal control), so hysterectomy does not lead to menopause.
It is important to clarify that hysterectomy does not directly alter a woman's feminine identity or ability to experience sexual pleasure.
Most women report improvements in their sex lives, especially if the surgery has resolved the conditions that previously caused excessive bleeding and pain. Only in some cases may temporary alterations occur due to the recovery process.
Substantiated information by:

Published: 14 January 2022
Updated: 11 July 2025
Subscribe
Receive the latest updates related to this content.
Thank you for subscribing!
If this is the first time you subscribe you will receive a confirmation email, check your inbox