



26 September 2025
PortalClinic home
Joint project with
BBVA Foundation website.This link opens in a new tab.
What is Sleep Apnoea?
Reading time: 3 min
Obstructive Sleep Apnoea (OSA) is a disease characterised by excessive daytime sleepiness, snoring and repeated episodes of reduced or interrupted breathing during sleep, known respectively as hypopnoea and apnoea.
Sleep Apnoea explained in first person
Professionals and patients explain how you live with the disease
Sleep apnoea | PortalCLÍNIC
To anyone who is snoring and who has apneas observed by the bed partner or sleepiness during the day, you must consult your primary care doctor, and know that the treatment of this disorder will improve your quality of life and your night rest.
Cristina Embid
Pneumologist
Sleep Apnoea explained in first per...
The CPAP changed my life, because now I wake up and I feel happy and content. I'm not tired and I can do things. Above all, I’m not always falling asleep.
Carme
Patient
These episodes of reduced or interrupted breathing during sleep are accompanied by a reduction in blood oxygen levels and conclude with a brief awakening (arousal) which leads to unrefreshing sleep.
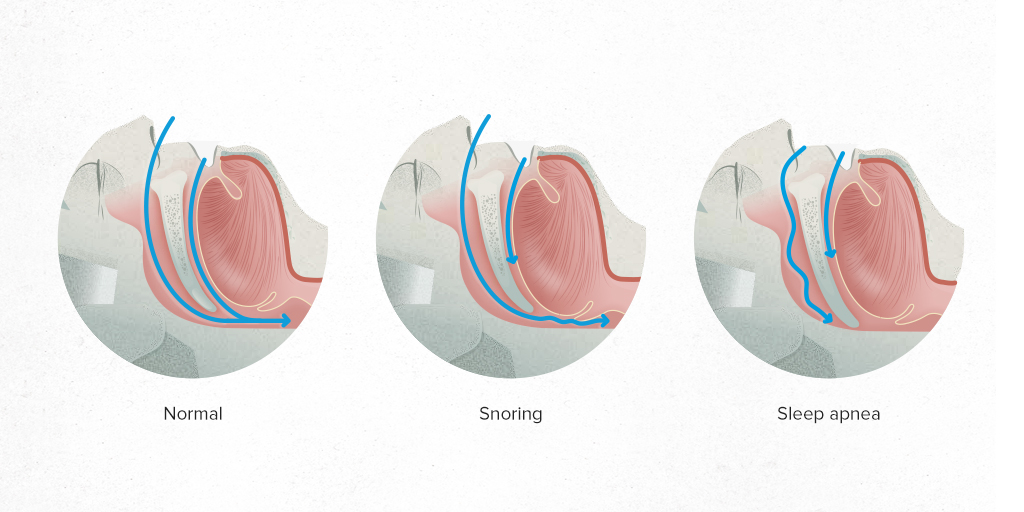
The mechanism responsible for producing these episodes during sleep is an imbalance between the strength of the upper airway dilator muscles (genioglossus and hyoglossus) and the “collapsing” muscles (diaphragm), due to certain anatomical and/or functional predispositions.
People who have obstructive sleep apnoea can develop cardiovascular, neurocognitive, respiratory, inflammatory and metabolic disorders due to these repeated episodes of total or partial collapse of the upper airway.
Types of Sleep Apnoea
There are three different types of apnoea and hypopnoea:
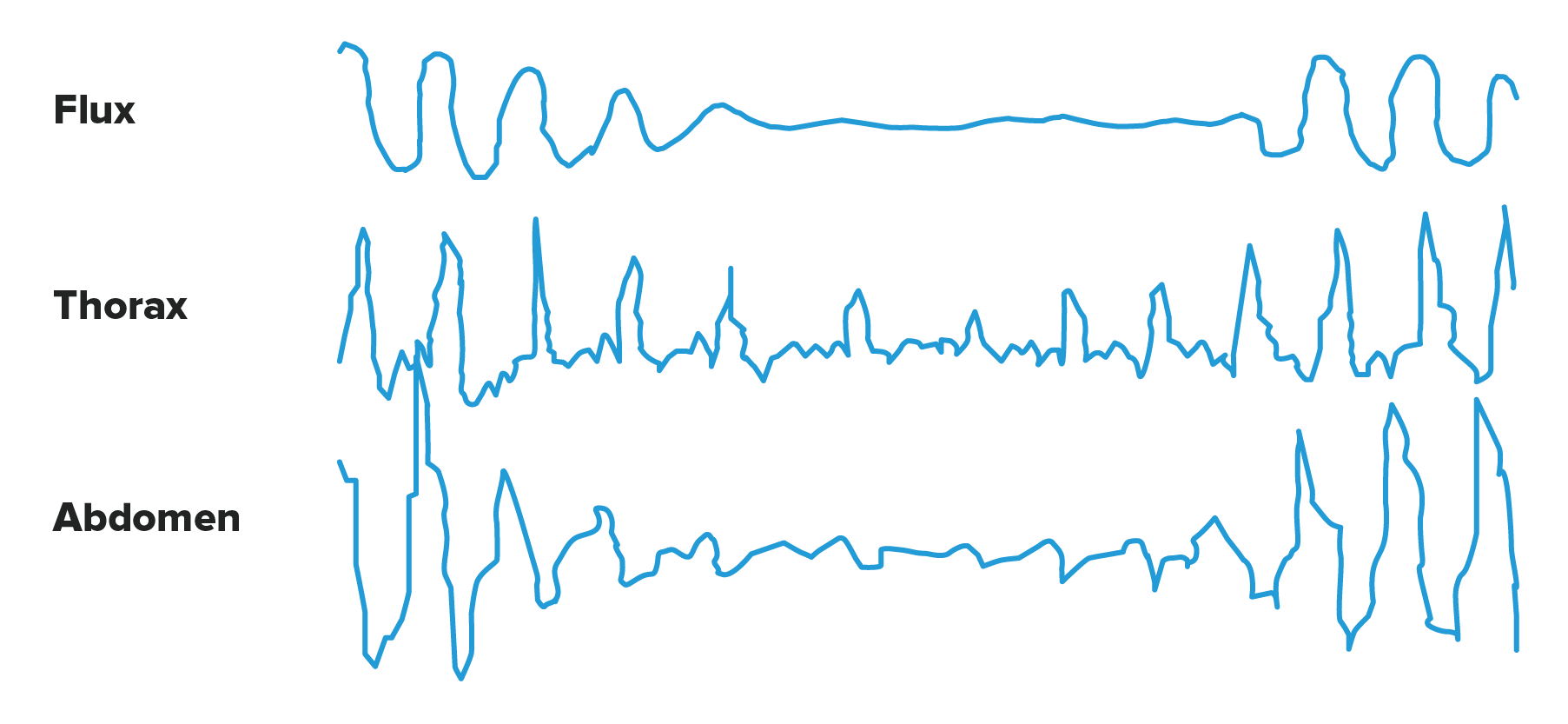
Apneas obstructivas. Son las más frecuentes. Se caracterizan por el cese o la disminución del flujo aéreo en la boca y/o la nariz, a pesar de los esfuerzos de la musculatura ventilatoria que lucha contra una obstrucción situada en la región faríngea.
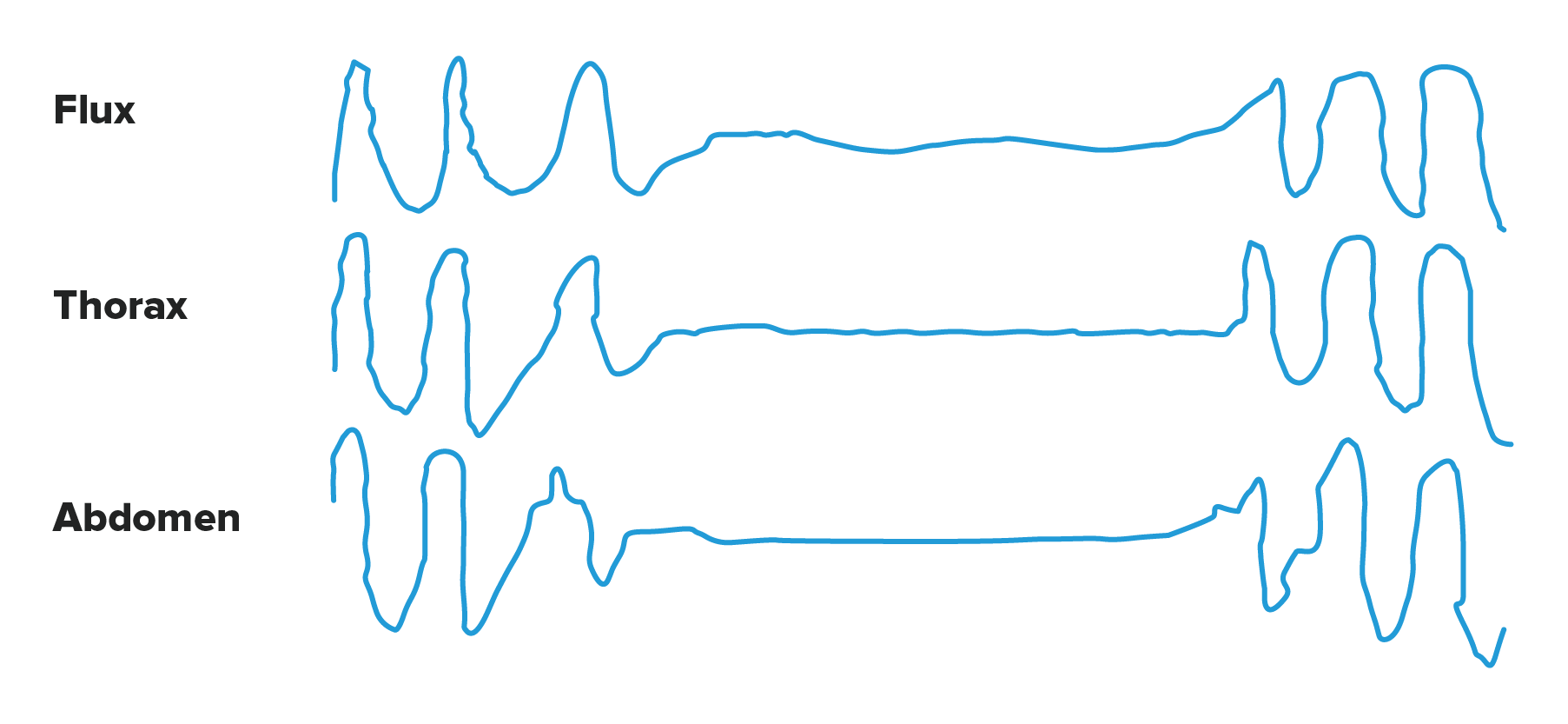
Central apnoea. The cessation or decrease in nasal-buccal airflow is accompanied by a pause or reduction in respiratory muscle activity due to a decline in the activity of the brain’s respiratory centre.
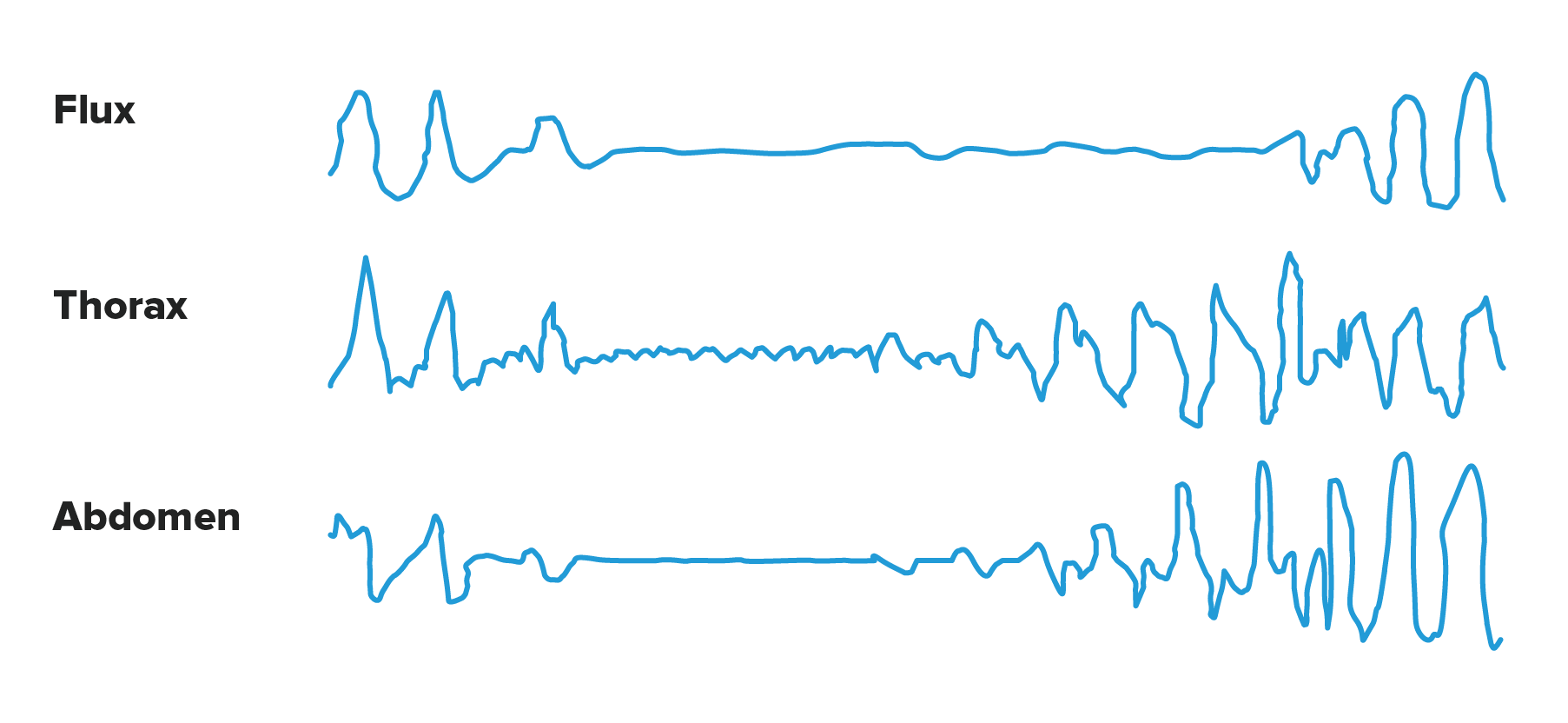
Mixed apnoea. The apnoea is initially central and subsequently obstructive.
When it comes to obstructive sleep apnoea (OSA), the condition predominantly involves hypopnoea and obstructive apnoea. Central apnoea is less common and may appear in a physiological form when transitioning to sleep in healthy people, but it may be pathological in patients with Central Nervous System (CNS) disorders or heart diseases that affect their control over their breathing.
Sleep Apnoea cycle
The sequence of events that occur throughout the night in patients with obstructive sleep apnea gives rise to a series of pathophysiological changes which are responsible for the main symptoms associated with the illness.
The same cycle is always repeated: sleep, apnea, changes in the concentration of oxygen and carbon dioxide in the blood (gasometric changes), transient awakening and end of apnea.
Repeated gasometric changes cause pulmonary and systemic vasoconstriction, leading to systemic and pulmonary arterial hypertension. These conditions may increase the risk of cardiovascular diseases such as heart disease or cerebrovascular accidents in these patients. The association with arrhythmias is common, particularly episodes of atrial fibrillation. In severely obese individuals, nocturnal gasometric changes may contribute to the development of chronic daytime hypoventilation.
Current evidence shows that hypoxia-reoxygenation phenomena (oxygen deprivation and reoxygenation), secondary to apnea-hypopnea events and their termination, are responsible for oxidative stress (cell aging and damage), the release of inflammatory products, and cell death (apoptosis).
Furthermore, repeated transient awakenings are responsible for sleep fragmentation, which accounts for most neuropsychiatric manifestations, such as daytime sleepiness and cognitive disorders.
Scientific evidence has established that obstructive sleep apnea (OSA) is an independent risk factor for developing cardiovascular diseases, particularly arterial hypertension, cerebrovascular disease, arrhythmias, and heart failure. Additionally, it is associated with an increased rate of traffic accidents. The independent relationship between OSA and diabetes mellitus and metabolic syndrome has also been demonstrated.
How many people are affected by Sleep Apnoea?
Its prevalence among the adult population is around 6–13% and this increases with age. It is two to three times more common in men than in women, although the number of women affected increases significantly after menopause.
Around two million people in Spain have obstructive sleep apnea, although less than 10% of those affected are correctly diagnosed and treated.
PortalClinic home
Joint project with
BBVA Foundation website.This link opens in a new tab.
Sorry this content wasn't helpful to you. Send us your comment and we will take it into account to continue improving.
Thanks for your help!
An error has occurred and we were unable to send your opinion, please try again later.
Substantiated information by:
Concepción Ruiz Sánchez
Advanced Practice Nurse
Pneumology Service
Cristina Embid López
Pneumologist
Pneumology Service
Josep M. Montserrat Canal
Pneumologist
Pneumology Service
Mireia Dalmases Cleries
Pneumologist
Pneumology Service
Published: 16 January 2020
Updated: 25 March 2025
The donations that can be done through this webpage are exclusively for the benefit of Hospital Clínic of Barcelona through Fundació Clínic per a la Recerca Biomèdica and not for BBVA Foundation, entity that collaborates with the project of PortalClínic.
Subscribe
Receive the latest updates related to this content.
Thank you for subscribing!
If this is the first time you subscribe you will receive a confirmation email, check your inbox
An error occurred and we were unable to send your data, please try again later.

