Treatment of liver cancer
The choice of treatment depends on several factors, such as the stage of the tumor (for hepatocellular carcinoma, according to the BCLC system), the presence of other diseases, and specific technical aspects of each treatment, for example, the location of the lesion.
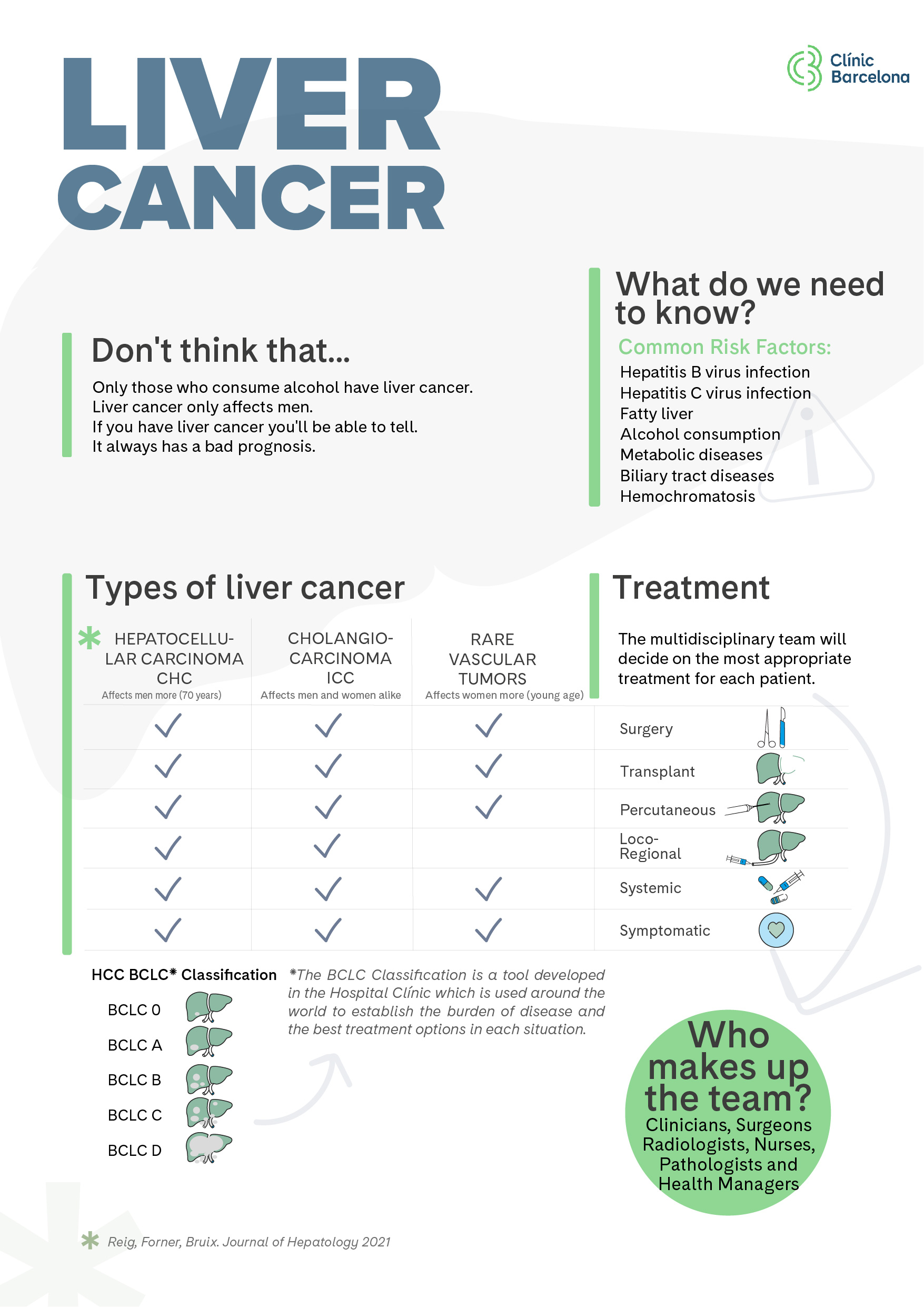
Once liver cancer is diagnosed, a multidisciplinary team reviews each case with the goal of offering the most optimal therapeutic option for each individual, with the overarching objective of increasing survival in all cases.
The multidisciplinary team is composed of all the professionals directly involved in the diagnosis and treatment of this tumor: hepatologists, radiologists (including interventional radiology specialists), nuclear medicine specialists, hepatobiliary surgeons, pathologists, medical oncologists, and radiation oncologists, as well as nursing staff and social workers involved in the care process.
Liver surgery, also known as surgical resection, involves removing the part of the liver that contains the tumor. It is a curative treatment option and is mainly indicated for individuals in good general condition, with adequate liver function and no spread of the cancer outside the liver. The decision to perform a resection depends on the location of the tumor, its size, the number of lesions, and whether the remaining liver will be able to function properly.

Laparoscopic surgery. This is a minimally invasive surgical technique performed through small incisions. This approach helps reduce postoperative pain and respiratory complications, improves cosmetic outcomes, and enables faster recovery. Studies have shown that survival outcomes are similar to those achieved with conventional surgery, making it the preferred approach. Whether this type of surgery can be performed depends on the location of the tumor.

Laparotomic surgery. This type of surgery requires a large incision in the abdomen, from which recovery is usually slower. In many cases, particularly when dealing with tumours located in posterior segments of the liver or which need an extensive resection, it is the only viable treatment option.
This type of procedure cannot be performed in all individuals, as the tumor often arises in a liver already affected by cirrhosis. In such cases, extensive resections are not feasible due to the risk that the liver may not function properly after surgery. If the patient has cirrhosis without impaired liver function, a careful assessment is required to evaluate the risk of liver decompensation or postoperative complications.
One of the key parameters to assess is the presence of portal hypertension (increased pressure in the portal vein, which delivers nutrient-rich blood from the stomach and intestines). This parameter is closely related to the degree of liver fibrosis and the severity of cirrhosis, and it is essential for identifying ideal candidates for surgical resection.
In well-selected cases, liver resection is very safe (perioperative mortality below 1%) and offers a five-year survival rate of over 70% in patients with hepatocellular carcinoma, and 40–50% in those with cholangiocarcinoma. Despite strict candidate selection and excellent survival outcomes, the recurrence rate after complete resection remains very high, reaching 50–70% at five years.
To date, no treatment has proven effective in preventing tumor recurrence. Therefore, close follow-up of all patients who have undergone liver cancer surgery is crucial, with the aim of detecting tumor recurrence early and offering effective additional treatments.
Common postoperative complications of liver cancer surgery are infections (especially surgical wound and respiratory infections), abdominal fluid retention (ascites) and a deterioration in liver function, which is rare and usually only temporary.
In the long term, people may suffer from mild pain and hypersensitivity at the incision site and, in some cases, an eventration (hernia) of the incision.
In hepatocellular carcinoma, liver transplantation is the treatment of choice for individuals with impaired liver function and a limited tumor burden (based on the number and size of the tumors). It is especially indicated when liver function is insufficient to allow for other treatment options.
The possibility of undergoing liver transplantation is limited by the risk of tumor recurrence, that is, the tumor returning after transplant. Therefore, it is essential to carefully select patients who are most likely to benefit from the procedure. The risk of recurrence depends primarily on tumor burden: the larger the tumor or the more nodules present, the higher the risk. As a result, strict limits on the number and size of lesions are set, and not everyone with hepatocellular carcinoma qualifies for transplantation.
Liver transplantation has the advantage of being a highly effective treatment that can completely eliminate the tumor while also curing the underlying chronic liver disease. However, following the transplant, lifelong medication is required to prevent rejection of the transplanted organ. This immunosuppressive therapy comes with long-term side effects and requires ongoing medical monitoring.
Cholangiocarcinoma is generally considered a contraindication for liver transplantation due to the high risk of post-transplant recurrence. Only in highly selected cases can transplantation be considered, and only when outcomes are expected to be comparable to those of hepatocellular carcinoma.
It is the treatment of choice for individuals with early-stage hepatocellular carcinoma when surgical resection is not possible or liver transplantation is contraindicated.
Tumor ablation can be performed by directly instilling chemical substances, mainly ethanol, into the tumor, or by modifying the tumor’s internal temperature, as in the case of radiofrequency or microwave ablation. Another method of ablation is through radiotherapy.
Currently, radiofrequency ablation (RFA) is considered the standard technique. This treatment is ultrasound-guided and involves inserting a thin, needle-like probe through the skin into the tumor. A high-frequency electrical current is then passed through the tip of the probe, which heats the tumor and destroys the cancer cells. It is a very safe treatment, typically requiring only one day of hospitalization, and it is highly effective for tumors smaller than three centimeters offering results comparable to surgical resection in patients with solitary tumors of two centimeters.
The feasibility of this therapeutic approach depends largely on the tumor’s location and patient characteristics. In some cases, the lesion may be difficult or risky to access, which requires considering other treatment options. As with surgical resection, the main drawback of percutaneous ablation is the high likelihood of recurrence even when the tumor appears to have been completely eradicated initially.
In cholangiocarcinoma, ablation is also possible in a specific group of patients those with small tumors located within the liver for whom surgical resection is not feasible.
Chemoembolization, also known as TACE (Transarterial Chemoembolization), is the treatment of choice for patients with intermediate-stage hepatocellular carcinoma who have preserved liver function.
This procedure involves injecting a chemotherapeutic agent directly into the tumor (or tumors, depending on the case). Additionally, the arterial blood flow feeding the tumor is blocked using a coagulant substance, helping to limit tumor growth.
TACE typically requires a hospital stay of about two days. Although it is generally well tolerated, it can cause side effects such as abdominal pain, fever, nausea, and vomiting in the days following the procedure. To achieve maximum effectiveness, the treatment is usually repeated several times at spaced intervals.
As with surgical resection and ablation, the main drawback of TACE is that most patients experience disease progression despite an initially good response. Therefore, close follow-up is essential in all cases.
In the case of cholangiocarcinoma, its efficacy has not been demonstrated, so it is not a recommended treatment.
Radioembolisation, also known as selective internal radiation therapy (SIRT), is a treatment which targets the tumour. It consists of releasing small radioactive-loaded beads (usually with yttrium-90) directly inside the tumour, through the artery feeding it.
This treatment can be especially useful in people with single tumours who cannot be operated upon, provided there is no invasion of other organs. The patient must also have good liver function and be in good general health. The treatment is done in two phases: the first is an individual treatment plan and the second is the actual treatment.
In hepatocellular carcinoma, conventional chemotherapy has not shown a significant survival benefit and has been associated with side effects, so its use is not recommended.
The most significant therapeutic breakthrough has come from the combination of immunotherapy and antiangiogenic therapies, such as atezolizumab (which helps the immune system recognize the cancer) combined with bevacizumab (which blocks the formation of new blood vessels that feed the tumor). Also effective are combinations of two immunotherapies, such as tremelimumab with durvalumab or ipilimumab with nivolumab, which work by activating different parts of the immune system to fight cancer, particularly in patients with advanced-stage hepatocellular carcinoma.
These new therapies have significantly improved life expectancy in people with advanced hepatocellular carcinoma. Without treatment, the median survival is about 8 months, while with these new therapies, survival can exceed 2 years.
In addition, these treatments open the door to other therapeutic options if the first-line treatment is ineffective or poorly tolerated. Currently, there is no validated second-line treatment when immunotherapy cannot be continued, so alternative options are mainly found in clinical trials.
In intrahepatic cholangiocarcinoma, important advances have also been made with the introduction of immunotherapy. One such option is the combination of durvalumab (a drug that helps the immune system attack cancer) with chemotherapy (Gemcitabine and Cisplatin).
Moreover, targeted therapies have also been introduced, treatments specifically designed to act on precise genetic alterations in the tumor. Some examples include pemigatinib (an FGFR inhibitor), ivosidenib (an IDH1 inhibitor), and pembrolizumab (an anti-PD-1 antibody). These personalized options allow for treatment to be tailored to each patient’s molecular profile.
Substantiated information by:




Published: 13 May 2020
Updated: 17 July 2025
Subscribe
Receive the latest updates related to this content.
Thank you for subscribing!
If this is the first time you subscribe you will receive a confirmation email, check your inbox



{kind=link}