







14 May 2025
PortalClinic home
Joint project with
BBVA Foundation website.This link opens in a new tab.
Treatments for Chronic Kidney Disease
Reading time: 4 min
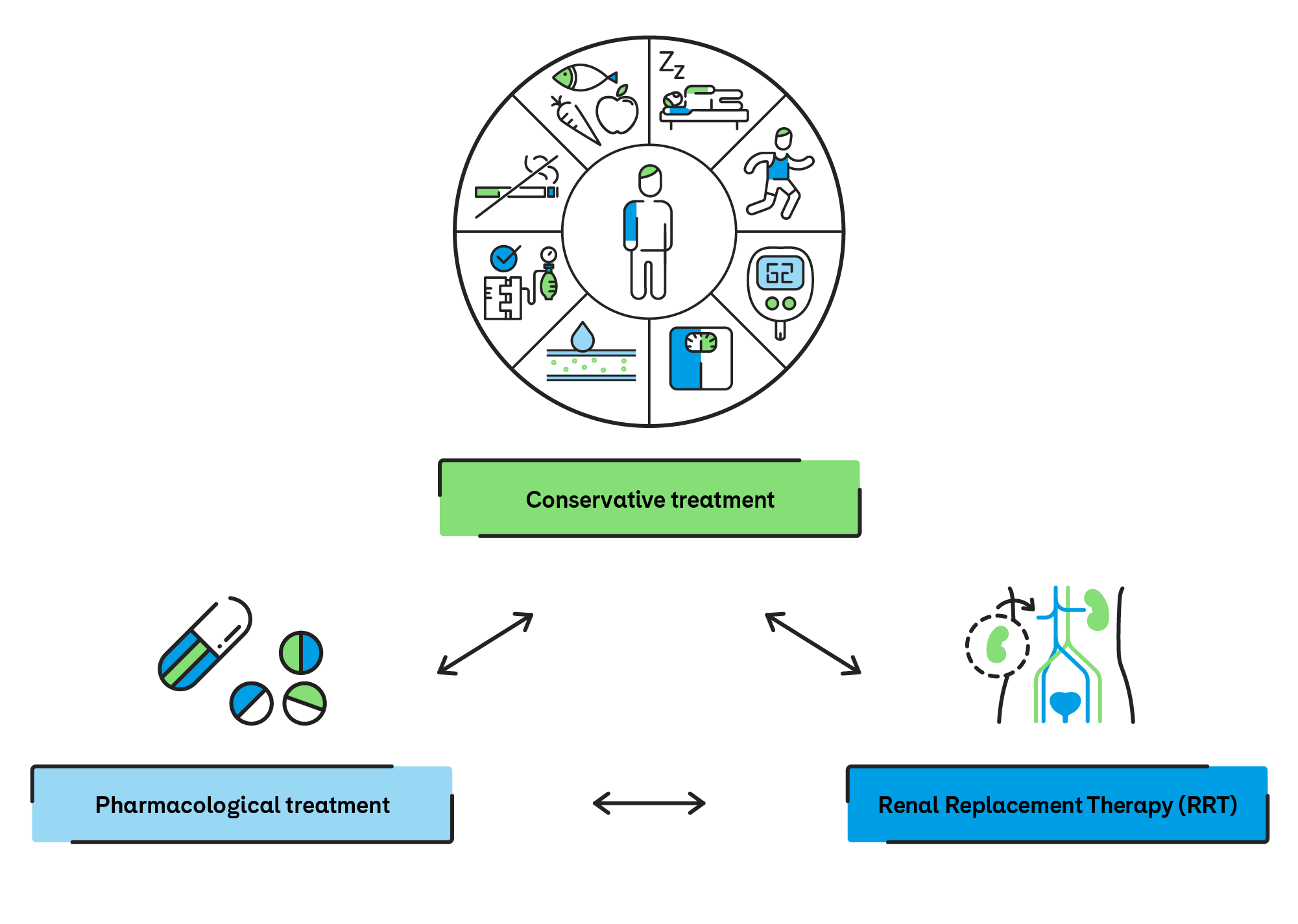
The treatment of chronic kidney disease (CKD) is based on strategies aimed at slowing disease progression, managing its complications and, in advanced stages, replacing kidney function through renal replacement therapies.
The choice of treatment depends on the stage of CKD, comorbidities, patient preferences and functional status. Decision-making should be shared among the patient, the family and the nephrology team. Guidelines recommend evaluating clinical, functional, psychosocial factors, as well as patient preferences.
Pharmacological treatment of chronic kidney disease (CKD) aims to control associated complications, slow the progression of renal impairment and improve the patient’s quality of life. A combination of medications is used to achieve this, tailored to the stage of the disease and the individual characteristics of each patient:
- Sodium–glucose cotransporter 2 inhibitors (SGLT2 inhibitors): these have been shown to reduce CKD progression and cardiovascular risk in patients both with and without diabetes.
- Diuretics: used to manage fluid retention and hypertension.
- Phosphate binders: essential for preventing disturbances in bone–mineral metabolism associated with CKD.
- Calcium and vitamin D supplements: indicated to maintain bone health and prevent secondary hyperparathyroidism.
- Erythropoietin or erythropoiesis-stimulating agents (ESAs) (stimulates the production of red blood cells): used to treat anaemia secondary to kidney disease.
- Potassium binders: help prevent and treat hyperkalaemia, a potentially serious complication of CKD.
- Antihypertensive therapy: angiotensin-converting enzyme inhibitors (ACE inhibitors) or angiotensin II receptor blockers (ARBs) are the first-line options due to their protective effects on the kidneys and cardiovascular system.
This comprehensive approach is always carried out under specialist supervision, with regular treatment adjustments to ensure maximum efficacy and safety.
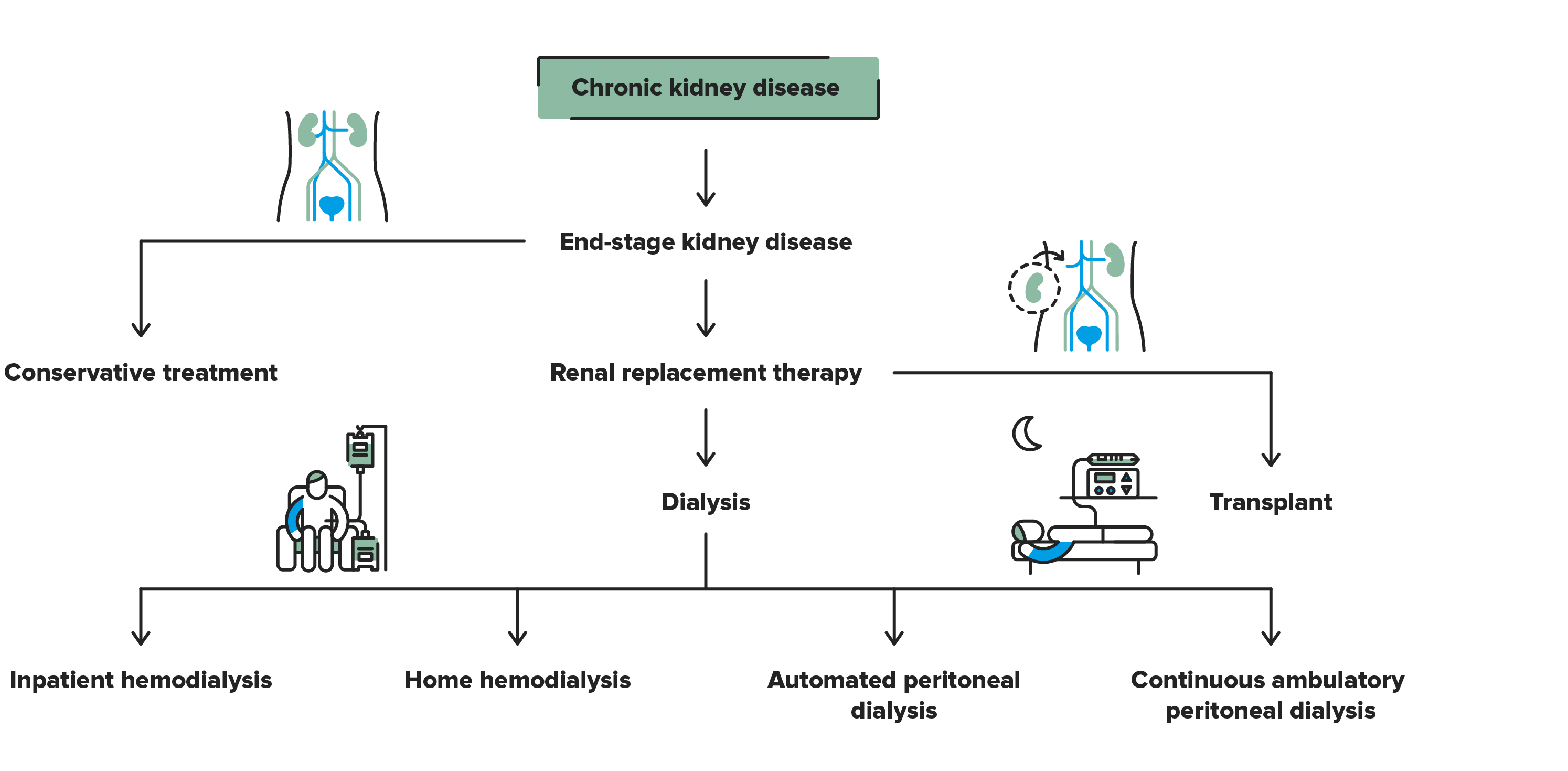
RRT is recommended when the glomerular filtration rate falls below 10–15 mL/min/1.73 m²—indicating kidney failure—or when uremic syndrome develops. There are three main modalities: a kidney transplant, haemodialysis and peritoneal dialysis.
This is the treatment of choice for patients with advanced CKD who have no contraindications. A functioning kidney graft offers better survival and quality of life compared to dialysis.
There are two types of transplants:
- Living donor: the kidney comes from a healthy individual who voluntarily donates the organ. Prior to donation, different medical studies are performed on the donor and the recipient to confirm the viability of the donation and the compatibility between both individuals. Outcomes are generally better and an additional advantage is the possibility of pre-emptive transplantation without the need for dialysis.
- Deceased donor: requires time on a transplant waiting list, which in Spain averages over two years.
In 2025, approximately 55% of patients receiving renal replacement therapy in Spain were living with a transplanted kidney.
Dialysis is a treatment that partially replaces kidney function by removing toxins and excess fluids. In 2025, more than 40% of patients receiving renal replacement therapy (RRT) were on dialysis, and around 30% were using some form of home therapy.
There are two main techniques: haemodialysis and peritoneal dialysis.
- Haemodialysis (HD). This type of dialysis requires vascular access (arteriovenous fistula [AVF] or a tunnelled catheter). It can be performed in a centre or at home. Home haemodialysis has increased due to compact machines, remote monitoring and more flexible treatment schedules.
- Standard sessions: 3 times a week, 4 hours per session.
- Advanced modalities: short daily HD or nocturnal home HD.
- Peritoneal Dialysis (PD). This technique uses the peritoneum as a filtering membrane to remove excess fluids and toxins from the body. It is the most common home dialysis modality. Its main advantage is that it offers greater autonomy and facilitates travel and work life.
It refers to comprehensive medical care without dialysis or a kidney transplant. Its main objective is to control disease progression, relieve symptoms and preserve the best possible quality of life, according to the needs and preferences of each individual.
The approach is particularly appropriate for patients with severe comorbidities, advanced age or significant functional limitations, for whom renal replacement therapies may not provide a clear or desired benefit.
Conservative management includes:
- Blood pressure control, essential to slow the progression of kidney damage and reduce cardiovascular risk.
- Comprehensive management of associated conditions, such as diabetes, obesity and dyslipidaemia, through pharmacological treatment and lifestyle modifications.
- Treatment of CKD-related metabolic complications, including anaemia, hyperkalaemia, metabolic acidosis and mineral and bone metabolism disorders.
- Supervised nutritional support, with individualised dietary recommendations to maintain adequate nutritional status and prevent complications.
- Active symptom management, including fatigue, pruritus, nausea, pain and sleep disturbances, with an approach focused on overall patient well-being.
This type of treatment is always delivered under specialist follow-up, with coordinated, person-centred care that allows clinical decisions to be aligned with disease progression and patient values.
PortalClinic home
Joint project with
BBVA Foundation website.This link opens in a new tab.
Sorry this content wasn't helpful to you. Send us your comment and we will take it into account to continue improving.
Thanks for your help!
An error has occurred and we were unable to send your opinion, please try again later.
Substantiated information by:
Anna Yuguero
Physiotherapist
Nephrology Department
Bárbara Romano Andrioni
Dietitian - Nutritionist
Endocrinology and Nutrition Department
Manel Vera Rivera
Nephrologist
Nephrology Department
Marta Quintela Martínez
Nurse
Nephrology Department
María Teresa López Alonso
Nursing of Vascular Access
Nephrology Department
Montserrat Monereo Font
Social Worker
Nephrology Department
Ángeles Mayordomo Sanz
Peritoneal Dialysis Nurse
Nephrology Department
Published: 20 February 2018
Updated: 3 June 2026
The donations that can be done through this webpage are exclusively for the benefit of Hospital Clínic of Barcelona through Fundació Clínic per a la Recerca Biomèdica and not for BBVA Foundation, entity that collaborates with the project of PortalClínic.
Subscribe
Receive the latest updates related to this content.
Thank you for subscribing!
If this is the first time you subscribe you will receive a confirmation email, check your inbox
An error occurred and we were unable to send your data, please try again later.

